Why “Stand Up Straight” Doesn’t Work
Decoding Posture: Post 4
The spine is not meant to be straight. It’s a beautifully engineered series of curves designed to absorb load, distribute force, and allow fluid, adaptable movement. When we tell clients to “stand up straight,” we often push them away from their natural alignment and into bracing, gripping, and overcorrection.
Why the Spine Has Curves (and Why They Matter)
The spine’s curves are not flaws — they are functional architecture and essential for our health. Each curve plays a specific role:
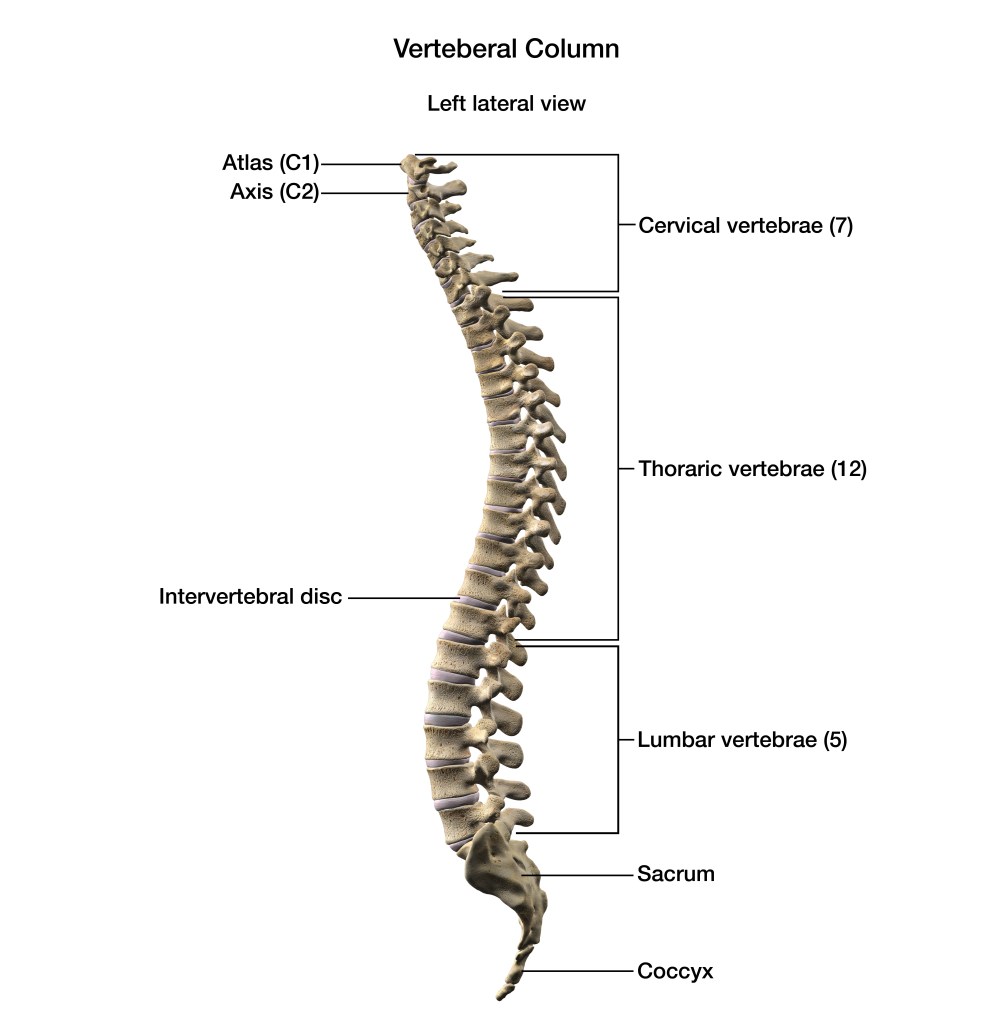
Cervical lordosis (neck curve)
- Positions the head over the body
- Allows shock absorption during walking and running
- Supports visual orientation and balance
Thoracic kyphosis (mid‑back curve)
- Protects the heart and lungs
- Allows rotation for gait, turning and reaching
- Helps distribute load through the ribcage
Lumbar lordosis (lower‑back curve)
- Supports upright posture
- Allows hip–spine coordination
- Absorbs compressive forces during standing and lifting
Together, these curves create a spring-like system that manages load far better than a rigid, straight column ever could.
What Happens When Curves Are Too Much or Too Little?
Spinal curves naturally vary, but when they become exaggerated or flattened, the body often compensates elsewhere.
When curves are excessive
Examples:
- Hyperlordosis (excessive lumbar curve)
- Hyperkyphosis (excessive thoracic rounding)
Possible consequences:
- Lower‑back compression
- Facet joint irritation
- Ribcage collapse and restricted breathing
- Neck strain from forward head posture
- Hip flexor overactivity or gripping
When curves are reduced
Examples:
- Flat lumbar spine
- Reduced thoracic kyphosis
- Military or Flat Back posture
Possible consequences:
- Disc pressure increases
- Reduced shock absorption
- Overuse of superficial muscles
- Stiff, braced movement patterns
- Difficulty accessing natural spinal rotation
These patterns are not diagnoses — they’re simply observations that help us understand how someone moves, where muscle imbalances may be and how we can help our clients.
Why We Shouldn’t Guess or Label Clients
As movement professionals, we see patterns — but we do not diagnose.
Two people can look similar externally but have completely different underlying causes:
- One person’s hyperlordosis may be structural
- Another’s may be habitual
- Another’s may be a protective response to pain
- Another’s may be linked to breathing mechanics
This is why guessing is risky. It can lead to:
- Overcorrecting a pattern that doesn’t need correcting
- Giving exercises that aggravate symptoms
- Misinterpreting a structural variation as a “fault”
- Missing red flags that require medical input
A proper diagnosis — when needed — must come from a qualified clinician.
Our role is to observe, interpret movement, and guide clients safely, not to label or pathologise.
How to Spot Habitual Patterns
Look for subtle, consistent tendencies such as:
- A stiff or immobile thoracic spine
- A collapsed or rigid ribcage
- Excessive lumbar gripping
- A forward‑shifted ribcage
- A tucked or untucked pelvis influencing spinal curves
- Breath patterns that reinforce tension
- Where the weight is on the feet
These patterns tell a story — not about “good” or “bad” posture, but about how someone has adapted to their life, habits, and history.
If you want to learn how to interpret spinal patterns and understand the deeper relationships between breath, pelvis, gait, and spinal curves the Postural Assessment & Correction Course offers a practical, compassionate, research‑informed approach with lots of practical workshops.

Leave a comment